Is the presence of echo-rich periportal cuffing in the liver indicator
for abdominal inflammation in pediatric patients?
Nurdan Fidan1, Esra Ummuhan Mermi Yetis2, Muammer Murat1, Cuneyt Yucesoy3, Ebru
Turgal4, Mehmet Metin5



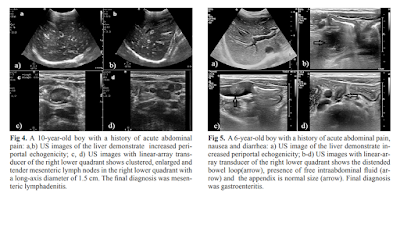


ErPC [echo rich periportal cuffing] appears especially in diseases
associated with abdominal inflammation such as gastroenteritis, acute
appendicitis, perforated appendicitis and mesenteric lymphadenitis. When
evaluated with adequate clinical information, the presence of ErPC is a
finding of high sensitivity and specificity in pediatric patients. This could
have a significant contribution to correct diagnoses by directing the
radiologists or clinicians to further examinations or follow-ups.
DÀY KHOẢNG CỬA: DẤU HIỆU SIÊU ÂM CỦA VIÊM TRONG Ổ BỤNG
MỤC TIÊU HỌC TẬP:
1/ Mô tả được hình ảnh siêu âm dày khoảng cửa và dấu trời sao khi
khám siêu âm gan
2/
Trình bày được các nguyên nhân và tình huống lâm sàng của dày khoảng cửa và dấu
trời sao trong siêu âm gan
3/ Phân tích được một số tình huống lâm sàng có dày
khoảng cửa và dấu trời sao
NỘI DUNG
1. DẪN NHẬP:
Đau bụng
là lý do để khám siêu âm bụng trong thực hành lâm sàng ngoài các cách khám lâm
sàng truyền thống. Tuy không là phương tiện chẩn đoán chính thống, siêu âm bụng
thường quy/tại giường/tiếp cận giúp định hướng chẩn đoán và cung cấp hình ảnh
bình thường và bệnh lý trong khoang bụng.
Gần
đây y văn siêu âm có những bài báo về đau bụng ở trẻ em và người lớn, trong đó
ghi nhận vài dấu hiệu siêu âm TRONG GAN như phản ứng quanh cửa [portal
reaction], dấu trời sao [starry sign appearance], dày quanh cửa [periportal
echo rich] trong một số bệnh lý như viêm gan, viêm dạ dày ruột, viêm ruột dư cấp…
Trong
bài này chúng ta sẽ mô tả và tìm hiểu các dấu hiệu siêu âm trên.
2. CÁC DẤU HIỆU SIÊU ÂM TRONG GAN CỦA ĐAU BỤNG:
A. PHẢN ỨNG QUANH CỬA [PORTAL REACTION]:
Là các đường echo rich cạnh khoảng cửa gan trên nền
nhu mô gan echo poor thường gặp trong viêm gan cấp (từ 10% đến 13.9% , n=1.367 ca)
được cho là các tế bào gan viêm phù nề làm tăng sáng quanh cửa ở trung tâm gan.
Dấu hiệu này có thể gặp trong các ổ bụng có hội chứng viêm các cơ quan khác như
dạ dày,ruột.
B. DDẤU TRỜI SAO [STARRY SKY APPEARANCE]:
Là các đường echo rich rải rác trong vùng ngoại biên
gan. Dấu hiệu này có thể gặp trong các ổ bụng có hội chứng
viêm các cơ quan như gan, dạ dày,ruột. Theo H Tchelepi -
2002, dấu hiệu này không có giá trị trong viêm gan
C. DÀY QUANH CỬA [PERIPORTAL ECHO RICH]:
Dấu hiệu này mới được công bố trong một bài báo siêu
âm ở trẻ em (2019). Tác giả không ghi nhận có trong viêm gan, chỉ có ở một số
trường hợp viêm trong ổ bụng ở trẻ em cả 2 dấu trời sao và dày khoảng cửa.
3. BÀN LUẬN:
Cả 3 dấu hiệu này đều ở khoảng quanh cửa trung tâm và
ngoại biên của gan. Đây là mô tả của siêu âm dựa vào phù hợp của chẩn đoán lâm
sàng sau cùng, chưa được chứng minh bằng các phương tiện chẩn đoán hình ảnh
khác.
Khi tìm thấy 3 dấu hiệu trên người làm siêu âm nên tìm
thêm các triệu chứng siêu âm bất thường ở gan, dạ dày, ruột, hạch trong ổ bụng
để giúp hướng chẩn đoán cho một trường hợp đau bụng trong thực hành lâm sàng.
TÀI LIỆU THAM KHẢO:
SIÊU ÂM CHẨN ĐOÁN TRONG VIÊM GAN, 1997, Nguyễn Thiện Hùng – Phan
Thanh Hải – Phạm Thi Thu Thủy Trung tâm Chẩn đoán Y khoa (MEDIC) Thành Phố Hồ
Chí Minh
SONOGRAPHY of DIFFUSE LIVER DISEASES, by H Tchelepi -
2002, www.jultrasoundmed.org/content/21/9/1023.full
STARRY SKY APPEARANCE
https://radiopaedia.org/articles/starry-sky-appearance-ultrasound-1
IS THE PRESENCE OF
ECHO-RICH PERIPORTAL CUFFING IN THE LIVER INDICATOR FOR ABDOMINAL INFLAMMATION
IN PEDIATRIC PATIENTS htps://www.medultrason.ro/medultrason/index.php/medultrason/article/view/1940










