SIÊU ÂM ĐÀN HỒI TRONG
NIỆU KHOA
NGUYỄN THIỆN HÙNG-
PHAN THANH HẢI, TRUNG TÂM Y KHOA
MEDIC HOÀ HẢO, Thành phố Hồ Chí Minh
Siêu âm vốn có vai trò quan trọng trong chẩn đoán bệnh niệu
khoa cấp và mạn tính như cơn đau quặn thận, xoắn tinh hoàn, chấn thương thận,
hoặc dùng theo dõi hồi lưu bàng quang niệu quản, đánh giá vô sinh, đo thể tích
nước tiểu tồn lưu và phát hiện ung thư. Tuy nhiên có một số mặt siêu âm có độ
chính xác chưa đủ tin cậy và phải được CT và MRI xác nhận.
Khám siêu âm không tốn kém chi phí và thời gian nhiều,
không ảnh hưởng tia xạ và theo lệ [routine] do bác sĩ và lịch khám lâm sàng. Với
công nghệ mới như siêu âm với chất cản âm hay siêu âm đàn hồi, các ứng dụng
siêu âm càng được mở rộng.
Bài này nhằm đề cập khái quát về siêu âm đàn hồi và vài ứng
dụng tại thành phố HCM từ 2004 đến nay.
ÁP DỤNG SIÊU ÂM ĐÀN HỒI TẠI TP HỒ CHÍ MINH:
Trên thị
trường thành phố hiện có các máy siêu âm để phân tích định tính và định lượng độ căng mô (tissue strain), độ cứng (stiffness). Phân làm 2 loại chính:
tĩnh [static] và động [dynamic].
*static= với nguồn kích thích cơ học trực tiếp: compression
elastography hay strain imaging, như máy Philips, GE, Hitachi với Hitachi
Real-Time Tissue Elastography (HiRTE).
*dynamic= với lực bức xạ (radiation force) gây ra đàn hồi thoáng qua [transient elastography].
- Transient elastography (như Fibroscan®)
- Supersonic Shear Imaging : với sóng biến dạng [shear wave] (như Supersonic Imagine Aixplorer)
- ARFI imaging: với xung lực bức xạ âm [Acoustic Radiation Force
Impulse (ARFI)] như Acuson Siemens S2000
Siêu âm đàn hồi phản ánh độ cứng của tổn thương, cách khám như siêu âm thường quy với đầu dò siêu âm có tích hợp kỹ thuật đàn hồi. Đã có nhiều bằng chứng trong y văn cho thấy siêu âm đàn hồi làm giảm việc sinh thiết không cần thiết, tăng cường chẩn đoán chính xác các bệnh lý u vú và gan.
Trung tâm Y khoa Medic Hoà Hảo hiện
đang sử dụng máy FibroScan (FS), máy Supersonic Imagine (supersonic
shear imaging, SSI) và máy Acuson S2000 (ARFI) cho các loại bệnh
lý tuyến vú, tuyến giáp, theo dõi xơ hoá gan, bệnh lý cơ khớp, phần mềm và da.
Trong Niệu khoa, có các lĩnh vực có đóng góp của siêu âm đàn hồi là nốt tinh hoàn, u thận, tiền liệt tuyến và theo dõi thải ghép thận.
1/ TINH HOÀN:
Với real-time elastography của máy Hitachi, Goddi và cs đã phân biệt các nốt và giả nốt (nodular/pseudonodular) của tinh hoàn bằng phần mềm cho điểm SC từ 1-5. Một báo cáo gồm 144 tổn thương của 88 tinh hoàn cho thấy 93,7% nốt lành tính có complete elastic pattern SC 1; 92,9% nốt lành tính nhỏ hơn 5mm và 100% tổn thương giả nốt cũng có SC 1; trong khi 87,5% nốt ác tính có SC 4-5 (cứng). RTE giúp phân biệt nốt lành tính và ác tính tốt hơn; có độ nhạy=87,5%, độ đặc hiệu=98,2% và độ chính xác là 95,8% khi phân biệt nốt tinh hoàn lành tính và ác tính. Tuy nhiên RTE ít có liên quan với những tổn thương lớn.

Trong Niệu khoa, có các lĩnh vực có đóng góp của siêu âm đàn hồi là nốt tinh hoàn, u thận, tiền liệt tuyến và theo dõi thải ghép thận.
1/ TINH HOÀN:
Với real-time elastography của máy Hitachi, Goddi và cs đã phân biệt các nốt và giả nốt (nodular/pseudonodular) của tinh hoàn bằng phần mềm cho điểm SC từ 1-5. Một báo cáo gồm 144 tổn thương của 88 tinh hoàn cho thấy 93,7% nốt lành tính có complete elastic pattern SC 1; 92,9% nốt lành tính nhỏ hơn 5mm và 100% tổn thương giả nốt cũng có SC 1; trong khi 87,5% nốt ác tính có SC 4-5 (cứng). RTE giúp phân biệt nốt lành tính và ác tính tốt hơn; có độ nhạy=87,5%, độ đặc hiệu=98,2% và độ chính xác là 95,8% khi phân biệt nốt tinh hoàn lành tính và ác tính. Tuy nhiên RTE ít có liên quan với những tổn thương lớn.

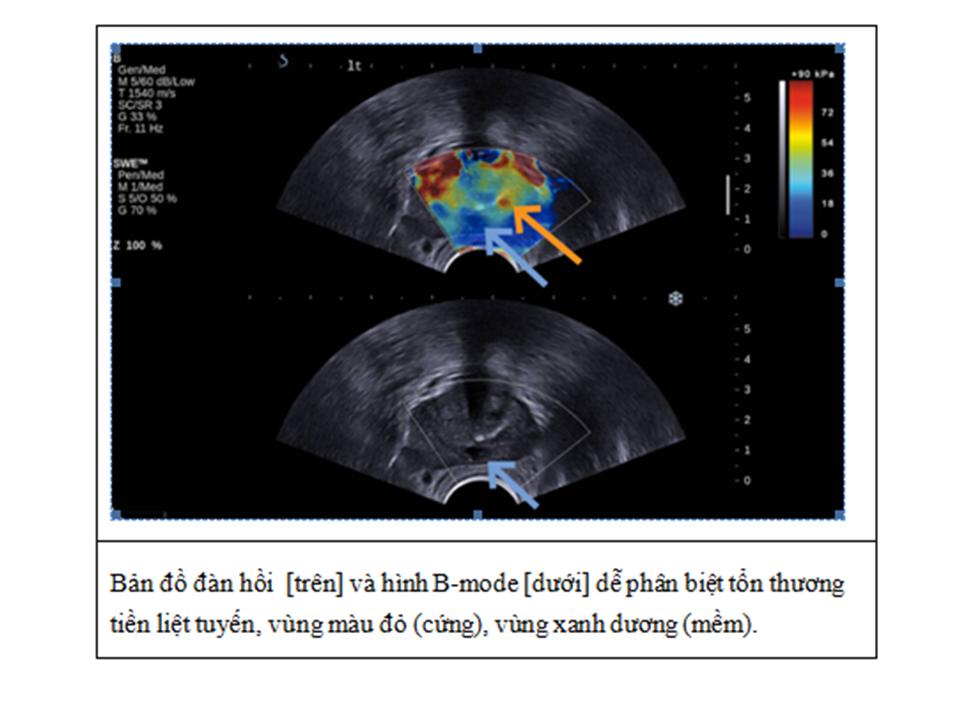
2/ TIỀN LIỆT TUYẾN= Siêu âm đàn hồi qua ngã trực tràng
- Real–time
Sonoelastography của máy
- Shear
Wave Elastography của máy Supersonic Imaging
Máy Aixplorer’s ShearWave
Elastography với đầu dò transrectal
dễ phát hiện các nhân tiền liệt tuyến. Bản đồ đàn hồi mã hoá màu định lượng
độ cứng tiền liệt tuyến hiển thị real–time và chỉ cần ấn 1 nút. Bản đồ giúp định
vị và phân biệt sự mất đồng dạng của tuyến tiền liệt và theo dõi sau điều trị
mà không phụ thuộc người khám và có tính lập lại. Ngoài ra có thể sinh thiết dựa
vào cùng lúc hình B-mode và hình đàn hồi, làm tăng độ chính xác của sinh thiết.
3/
BỆNH THẬN MẠN (CKD) và GHÉP THẬN
Số bệnh nhân bệnh thận mạn (chronic kidney disease, CKD) và tiếp sau đó là bệnh lý thận giai đoạn cuối (end-stage renal disease, ESRD), gia tăng và không được đánh giá đúng mức. Bệnh thận giai đoạn cuối tăng nhiều trong thập niên qua do các yếu tố tiên phát như cao huyết áp, tiểu đường, tăng lipid máu, béo phì hay nghiện thuốc lá.
Supersonic Shear Imaging (SSI) được chứng minh có khả năng theo dõi định lượng xơ hóa thận (kidney fibrosis) trên chuột và sau đó, được áp dụng trên người. Có các nghiên cứu với đầu dò cong và bản đồ đàn hồi nhày (viscoelastic properties) của thận người ghép ở cơ thể sống và đối chiếu với sinh thiết.
Một nghiên cứu theo dõi trong 8 tuần trên nhóm 50 chuột bị làm xơ hóa vi cầu thận (glomerulosclerosis) bằng L-Name nhằm khảo sát độ chính xác của kỹ thuật. Bản đồ đàn hồi định lượng của vỏ thận được thực hiện với đầu dò linear 8 MHz. Còn trên thận người ghép, bản đồ đàn hồi định lượng của vỏ thận được thực hiện với đầu dò cong 2,5MHz.
Kết quả
trên động vật cho thấy có sự gia
tăng độ đàn hồi vỏ thận từ 9-25kPa. Kết quả được đối
chiếu với mô học như tiểu đạm và/hoặc định lượng xơ hóa với 3 màu.
Trên thận người ghép có 3 nhóm được khảo sát: nhóm chứng, nhóm đối tượng thận ghép không hoạt động sớm và nhóm thận ghép không hoạt động muộn. Kết quả thu thập được ở 49 bệnh nhân với bản đồ đàn hồi ở sâu 8cm và rộng 10cm cho thấy độ đàn hồi thay đổi giữa các nhóm, tăng từ 9 đến 50kPa. Đối chiếu với mô học đạt được sự thống nhất về các dấu hiệu xơ hóa và độ đàn hồi. Như vậy, độ đàn hồi có liên quan với xơ hóa thận.
Trên thận người ghép có 3 nhóm được khảo sát: nhóm chứng, nhóm đối tượng thận ghép không hoạt động sớm và nhóm thận ghép không hoạt động muộn. Kết quả thu thập được ở 49 bệnh nhân với bản đồ đàn hồi ở sâu 8cm và rộng 10cm cho thấy độ đàn hồi thay đổi giữa các nhóm, tăng từ 9 đến 50kPa. Đối chiếu với mô học đạt được sự thống nhất về các dấu hiệu xơ hóa và độ đàn hồi. Như vậy, độ đàn hồi có liên quan với xơ hóa thận.

Vì hầu hết diễn tiến xơ hóa thận là do bệnh viêm thận mạn, việc xác định không xâm lấn và theo dõi diễn tiến này hẵn sẽ làm thay đổi dự hậu bệnh lý thận, nếu như bệnh nhân được áp dụng các điều trị trúng đích (targeted therapies).
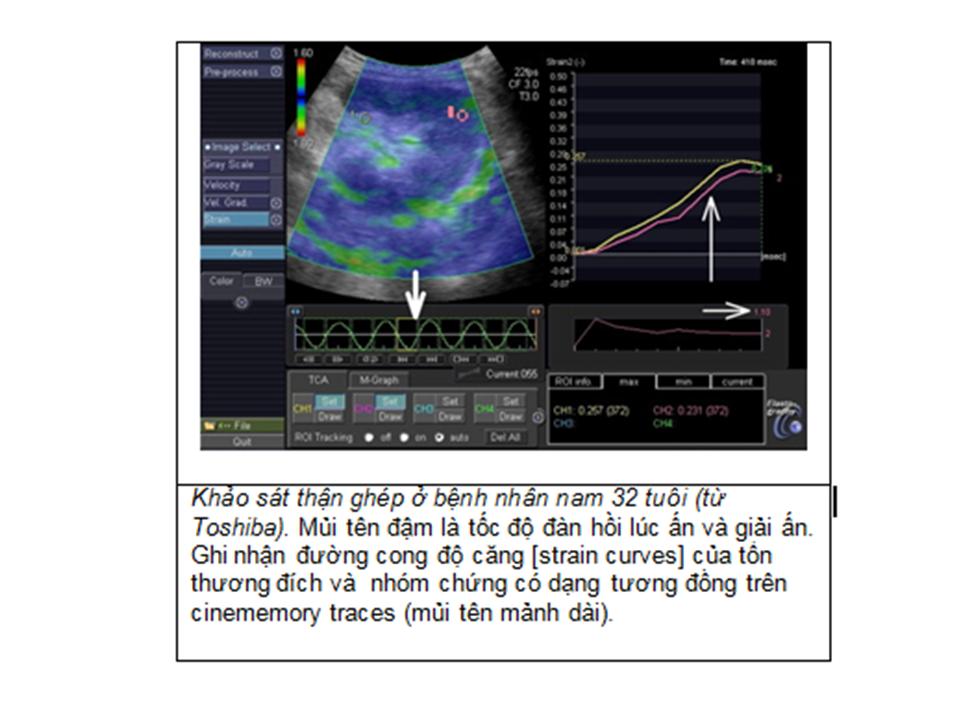
Với siêu âm đàn hồi ARFI của máy ACUSON S2000, gồm 2 kỹ thuật là VTQ (Virtual
Touch Tissue Quantification : đo định lượng tốc độ sóng biến dạng trong vùng khảo sát ROI,
tốc độ đàn hồi SWV [shear wave velocity] càng lớn mô thận ghép càng cứng do
fibrosis) và VTI (Virtual Touch Tissue
Imaging, định
tính độ cứng tương đối vùng ROI, tổn thương tối hơn [darker] mô xung quanh thì càng cứng hơn mô
xung quanh). Với giá trị cut-off của vận tốc đàn hồi VTQ chủ mô thận của thải ghép ở phần dưới (chỗ sinh thiết) SWV=2,81m/s, độ nhạy là 75% và độ đặc hiệu là 64,7%, ROC=0,78 với p=0,004 (Jeong Yeon Cho, 2010).
Kỹ
thuật siêu âm đàn hồi ARFI có vai trò
tiên lượng không xâm lấn trong bệnh thận thải ghép
thận mạn tính (chronic allograft nephropathy, CAN) do xơ hóa mô kẽ và teo ống thận (interstitial fibrosis and tubular atrophy) và theo dõi diễn tiến của xơ hoá mô kẽ và teo ống thận.

4/ U THẬN:
Dùng siêu âm đàn hồi ARFI để phân biệt carcinôm tế bào thận[renal cell carcinoma, RCC] với u AML [angiomyolipoma], Jeong Yeon Cho (2010), giả định RCC, đặc biệt là clear cell type, cứng hơn chủ mô thận và u AML. Ở 18 ca u thận nhỏ dưới 5 cm ở 16 bệnh nhân, với VTI chỉ số ratio of gray scales của khối u với vỏ thận (T/KG) và với VTQ, chỉ số ratio of SWVs của khối u với vỏ thận (T/KSWV) đều khác biệt.






Tóm lại, siêu âm đàn hồi mô, cả định tính--như với static
elastography--hoặc bằng cách sử dụng phương pháp dynamic để tracking (theo dõi)
sóng biến dạng, là kỹ thuật đàn hồi phong phú và phát triển nhanh, hứa hẹn cải
thiện chẩn đoán cho nhiều bệnh lý trong lĩnh vực niệu khoa và các chuyên khoa
khác. Tuy nhiên do còn non trẻ, kỹ thuật siêu âm đàn hồi cần được cân nhắc khi
áp dụng, thận trọng khi đọc kết quả để tránh những cạm bẫy do kinh nghiệm còn
ít.
Chú thích:
1. Shear Wave: sóng biến dạng, còn gọi là sóng ngang, là một biến dạng đàn hồi thẳng góc với hướng chuyển động của sóng.
Compression Wave: sóng đè nén, còn gọi là sóng dọc, là một đè nén vào môi trường.
2. Lực bức xạ âm (acoustic radiation force) là kết quả từ momentum transfer (chuyển đổi động lượng) từ sóng siêu âm lan truyền đến mô. Có các phương thức áp dụng lực bức xạ âm: tĩnh (static), thoáng qua (transient), hoặc có tính hoà âm (harmonically).
3. Elasticity Imaging Methods: Ngoài kích thích cơ học là chuyển động mô sinh lý (mạch đập), nếu=
- dùng nguồn rung động (vibration) từ ngoài để tạo sóng biến dạng trong mô= sonoelasticity.
- dùng nguồn nén tĩnh bên ngoài (external static compression) để kích thích cơ học = strain imaging.
- thuận tiện hơn 2 cách từ ngoài đã kể ở trên, dùng lực bức xạ âm (Sugimoto đề xuất đầu tiên, 1990) kết hợp trực tiếp trong mô = shear wave elasticity imaging (Sarvazyan và cs, Nightingale và cs, Bercoff và cs., Fink và cs).
4. Young's modulus= giá trị tuyệt đối đàn hồi Young, mô tả biến dạng theo chiều dọc với áp lực dọc.
5. Shear modulus= liên quan với biến dạng theo chiều ngang và được liên hệ với truyền sóng biến dạng trong môi trường đồng nhất đẳng hướng (isotropic homogeneous media).
6. Bulk modulus=của độ đàn hồi mô tả thay đổi thể tích của vật chất do kích thích từ ngoài.
1. Shear Wave: sóng biến dạng, còn gọi là sóng ngang, là một biến dạng đàn hồi thẳng góc với hướng chuyển động của sóng.
Compression Wave: sóng đè nén, còn gọi là sóng dọc, là một đè nén vào môi trường.
2. Lực bức xạ âm (acoustic radiation force) là kết quả từ momentum transfer (chuyển đổi động lượng) từ sóng siêu âm lan truyền đến mô. Có các phương thức áp dụng lực bức xạ âm: tĩnh (static), thoáng qua (transient), hoặc có tính hoà âm (harmonically).
3. Elasticity Imaging Methods: Ngoài kích thích cơ học là chuyển động mô sinh lý (mạch đập), nếu=
- dùng nguồn rung động (vibration) từ ngoài để tạo sóng biến dạng trong mô= sonoelasticity.
- dùng nguồn nén tĩnh bên ngoài (external static compression) để kích thích cơ học = strain imaging.
- thuận tiện hơn 2 cách từ ngoài đã kể ở trên, dùng lực bức xạ âm (Sugimoto đề xuất đầu tiên, 1990) kết hợp trực tiếp trong mô = shear wave elasticity imaging (Sarvazyan và cs, Nightingale và cs, Bercoff và cs., Fink và cs).
4. Young's modulus= giá trị tuyệt đối đàn hồi Young, mô tả biến dạng theo chiều dọc với áp lực dọc.
5. Shear modulus= liên quan với biến dạng theo chiều ngang và được liên hệ với truyền sóng biến dạng trong môi trường đồng nhất đẳng hướng (isotropic homogeneous media).
6. Bulk modulus=của độ đàn hồi mô tả thay đổi thể tích của vật chất do kích thích từ ngoài.
Tài liệu tham khảo chính:
1. Éric Bavu, Jean-Luc Gennisson, Mathieu Couade, Jeremy Bercoff, Vincent Mallet, Mathias Fink, Anne Badel , AnaÏs Vallet-Pichard, Bertrand Nalpas, Mickaël Tanter, Stanislas Pol: Noninvasive In Vivo Liver Fibrosis Evaluation Using Supersonic Shear Imaging: A Clinical Study on 113 Hepatitis C Virus Patients, Ultrasound in Medicine and Biology, Volume 37, Issue 9 , Pages 1361-1373, September 2011.
2. Stanislav Emelianov: Ultrasound Elasticity Imaging,University of Texas
3. Josef Jaros: Ultrasound Elastography,University of Kuopio , Finland
4. Andy Milkowski : Elasticity reaching Clinical Maturity, Siemens.
5. Mark L. Palmeri - Kathryn R. Nightingale: Acoustic Radiation Force-Based Elasticity Imaging Methods, Interface Focus (2011).
6. K J Parker, M M Doyley and D J Rubens: Imaging the elastic properties of tissue: the 20 year perspective, Phys. Med. Biol. 56 (2011).
7. Peter NT Wells, Hai Dong Liang: Medical Ultrasonic: Imaging of Soft Tissue Strain and Elasticity, J.R.Soc. Interface 16 June 2011.
1. Éric Bavu, Jean-Luc Gennisson, Mathieu Couade, Jeremy Bercoff, Vincent Mallet, Mathias Fink, Anne Badel , AnaÏs Vallet-Pichard, Bertrand Nalpas, Mickaël Tanter, Stanislas Pol: Noninvasive In Vivo Liver Fibrosis Evaluation Using Supersonic Shear Imaging: A Clinical Study on 113 Hepatitis C Virus Patients, Ultrasound in Medicine and Biology, Volume 37, Issue 9 , Pages 1361-1373, September 2011.
2. Stanislav Emelianov: Ultrasound Elasticity Imaging,
3. Josef Jaros: Ultrasound Elastography,
4. Andy Milkowski : Elasticity reaching Clinical Maturity, Siemens.
5. Mark L. Palmeri - Kathryn R. Nightingale: Acoustic Radiation Force-Based Elasticity Imaging Methods, Interface Focus (2011).
6. K J Parker, M M Doyley and D J Rubens: Imaging the elastic properties of tissue: the 20 year perspective, Phys. Med. Biol. 56 (2011).
7. Peter NT Wells, Hai Dong Liang: Medical Ultrasonic: Imaging of Soft Tissue Strain and Elasticity, J.R.Soc. Interface 16 June 2011.
8.
Jeong Yeon Cho: Clinical values & feasibility of ARFI elastography in assessment of transplanted kidney ,
Department of Radiology, Seoul
National University
Hospital
9. K.F. Stock, B.S. Klein, M.T. Vo Cong,
C. Regenbogen, S. Kemmner, M. Büttner, S. Wagenpfeil, E. Matevossian, L.
Renders, U. Heemann, C. Küchle, ARFI-based tissue elasticity quantification and
kidney graft dysfunction: First clinical experiences, Clinical Hemorheology and
Microcirculation, Volume 49, Number 1-4 / 2011.
10.
Brian S. Garra,
Ultrasound Elasticity Imaging, © Applied Radiology,4-2011



























