Open-angle glaucoma
(OAG) is a chronic progressive optic neuropathy that is increasing in
prevalence worldwide. Currently, intraocular pressure is the only known
modifiable risk factor. With lowering of intraocular pressure, the proportion
of individuals who experience progression of visual field defects is reduced
but continues to occur in some individuals. Many other risk factors have been
identified, including decreased ocular perfusion pressure and decreased ocular blood
flow. Various imaging methodologies have shown an association between OAG and
altered blood flow in the various circulations: retrobulbar, retinal, optic
nerve head and choroidal. In addition, different morphological alterations have
been found to be associated with OAG. This review will cover the evidence that
supports the association between altered ocular blood flow and glaucoma.
Furthermore, it serves to describe the future methodologies that will assess
ocular metabolism, which will strive to move the field closer to definitively
understanding the effect of vascular changes on OAG.

Expert Commentary
The understanding
of glaucoma has come a long way from the identification of IOP as a risk factor
for glaucoma. Numerous other risk factors have been identified including
decreased OPP, decreased OBF, circadian fluctuations in vascular parameters and
vascular dysregulation. However, increased IOP continues to be the only
modifiable risk factor for the progression of glaucoma. The association between
altered OBF and glaucoma has been repeatedly defined; however, the
pathophysiologic effect of altered blood flow on glaucomatous damage remains to
be understood. Moreover, there are a lack of progression data for parameters
such as OPP and OBF. Owing to a lack of large-scale longitudinal clinical
trials, more evidence needs to be present before a recommendation can be made
about measuring OBF in a clinical setting. Some of the aforementioned studies
have small sample sizes and do not possess large statistical power, which could
cause confusion due to reduced reproducibility of the studies. OBF measurements
remain to be a research methodology to understand more about the
pathophysiology of glaucoma. Nevertheless, the use of the methodologies of to
assess OBF are continually providing more information that will be used to
further understand the pathophysiology of glaucoma.
From the use of CDI
for measuring retrobulbar vessels to SLO angiography measuring retinal and
choroidal circulations, the blood flow methodologies are each able to assess a
subset of the ocular circulation. However, none are comprehensive in their assessment
and a combination of the various methodologies must be used to thoroughly
analyze OBF. Furthermore, each methodology has its disadvantages, such as CDI’s
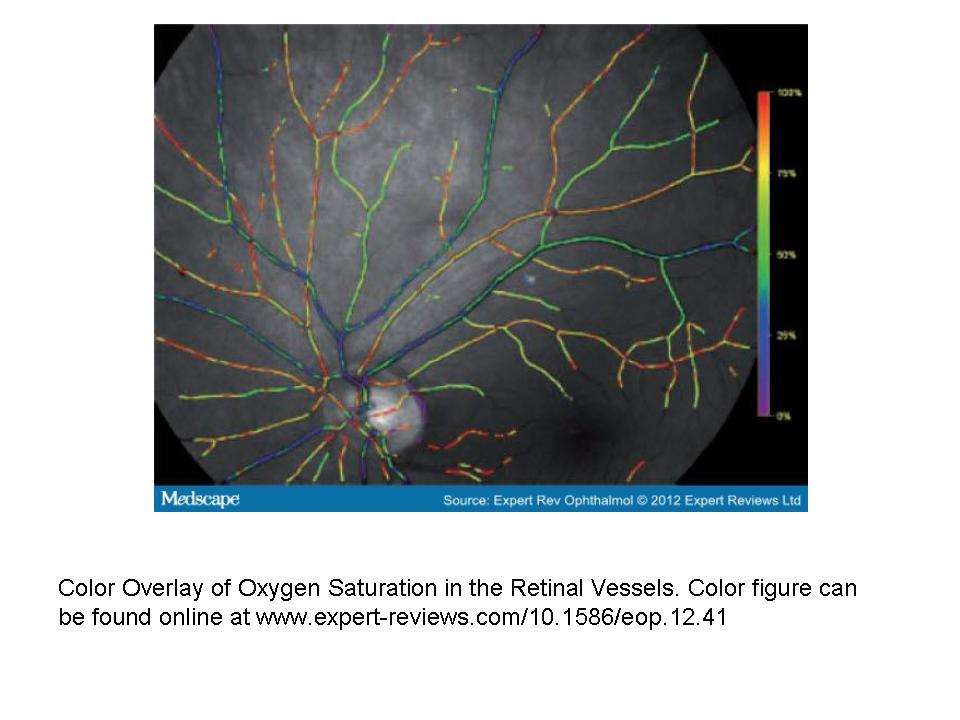
inability to measure blood flow volume. The relatively new technologies of
retinal oximetry and FD-OCT have shown promise to provide continued useful
information, with retinal oximetry’s ability to more directly measure tissue
metabolism and FD-OCT’s ability to provide accurate measurements of blood flow
in absolute units. For further usefulness of OBF data, a comprehensive and
standardized approach needs to be implemented.


Key Issues
- Intraocular pressure
is the only known treatable risk factor to decrease progression of
open-angle glaucoma.
- Sufficient evidence
exists from clinical trials to conclude that ocular blood flow deficits
are associated with glaucoma.
- Recent evidence has
shown that blood flow deficits lead to structural and functional damage.
- In large population
trials, decreased ocular perfusion pressure has been associated with the
prevalence and progression of glaucoma.
- Greater fluctuations
in ocular blood flow and ocular perfusion pressure have been shown to be
associated with the development of glaucoma and progression of visual field
loss.
- Currently, there is
insufficient evidence to conclude that insufficient blood flow directly
causes glaucoma progression.
- Future studies will
look at glaucoma progression as it relates to ocular blood flow parameters
in longitudinal studies involving an increased number of patients, and
more standardized methods.
- Assessment of blood
flow will need to move away from surrogate measurers of blood flow and
more towards measurement of oxygenation and metabolism of ocular tissues.